

Introduction Multiple myeloma (MM) is a kind of hematological malignancy which is characterized by high genetic heterogeneity. It has been proved that the existence and even the coexistence of numerical and structural cytogenetic abnormalities (CAs) play a critical role in the development and progression of MM. Hyperdiploidy (HD), as one of the two primary CAs of MM, can be observed in around half of the patients and is considered as a favorable prognostic factor. Nevertheless, its role in overcoming the negative effect of concomitant high-risk CAs remains controversial. Although the outbreak of novel drugs by the last decades, such as proteasome inhibitors (PIs) and Immunomodulatory drugs (IMiDs), has significantly improved the survival of patients, MM is still incurable and can relapse recurrently. The prognostic impact of HD in the era of novel agents and its impact on other CAs are unclear and under to be explored. Here, we report our results based on the Chinese population to provide some evidence for the above questions.
Methods A total of 213 patients between January 2013 to November 2017 were included in this study. All of the participants were from our database consisting of patients with newly diagnosed MM (NDMM) enrolled into the prospective, nonrandomized clinical trial (BDH 2008/02 or BDH 2014/03, all informed consents were obtained) approved by Institute of Hematology & Blood Diseases Hospital, Chinese Academy of Medical Science & Peking Union Medical College. According to patients' willingness and specific conditions, they were assigned to either PI- or IMiD-based inductive treatment and maintenance, with or without autologous stem cell transplantation (ASCT) as consolidation therapy. Bone marrow aspirate samples were collected before the initiation of therapy and MM cells were enriched by CD138 magnetic beads. Then fluorescence in situ hybridization (FISH) was performed. Specifically, if patients possessed at least an extra copy of probes for any two of chromosomes 5, 9, or 15 concurrently in more than 10% cells, they would be classified into HD subgroup; otherwise, they would be divided into NHD (non-hyperdiploidy) subgroup. Clinical and biological baseline characteristics were compared. Progression-free survival (PFS) and overall survival (OS) were measured using the log-rank test. Significant variables from the univariate analysis were selected for the cox stepwise regression analysis.
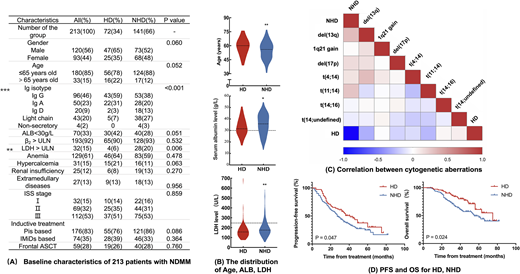
Results In our cohort, HD was identified in 34% (72/213) NDMM patients. HD was more common among older people (p=0.007). Patients with HD often had a lower level of serum albumin (p=0.037), but NHD patients had a higher frequency of elevated lactate dehydrogenase (LDH). Moreover, immunoglobulin isotype distribution was not similarly (p<0.001), in which patients with NHD were more often IgD or light chain isotype. As to the genetics aspect, 99.1% (211/213) patients harbored at least one CA, and NHD patients appeared to be more genetic instability. 14q32 (IGH) translocation(p<0.001), del(13q) (p<0.001) and del(17p) (p=0.012) were likely to be detected in patients with NHD. However, there were no significant differences in the ratio of 1q21 gain/amplification and complex karyotype. Among patients with IGH translocation, t(14;undefined) [could not find partner genes by t(4;14), t(11;14), t(14;16) or t(14;20) probes] and t(11;14) were the most common translocation type in HD and NHD patients respectively. Median follow-up was 37 (4-82) months, Patients with HD showed a better median PFS (41 months vs. 27 months, p=0.047) and median OS (75 months vs. 55 months, p=0.024). Further subgroup analysis showed that the prolonged survival of HD was significant in patients who did not receive ASCT as part of the first-line therapy, but it could not overcome negative prognostic effects of other CAs except complex karyotype. Multivariate analysis confirmed that the state of ploidy was an independent prognostic factor for MM.
Conclusions HD patients have specific differences in clinical and biological features. In the era of novel agents, MM patients with HD still have better survival than NHD. However, it may not ameliorate the adverse prognosis of concurrent high-risk CAs identified by FISH.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal